
CASE20210503_001
Presenter
Ivan Man Ho Wong
Authors
Ivan Man Ho Wong1
Affiliation
Queen Elizabeth Hospital, Hong Kong, China1
Valve - Aortic Valve
Transcatheter valve-in-valve procedure: Un-crossable bioprosthesis
Ivan Man Ho Wong1
Queen Elizabeth Hospital, Hong Kong, China1
Clinical Information
Patient initials or Identifier Number
K.K
Relevant Clinical History and Physical Exam
A 73-year-old female with history of surgical aortic valve replacement with a Perimount 2800 (Edwards Lifesciences, CA, USA) size 21 mm (true internal diameter 19 mm) was referred for valve-in-valve (VIV) with transcatheter aortic valve prosthesis in view of symptomatic, severe structural valve deterioration.
Relevant Test Results Prior to Catheterization
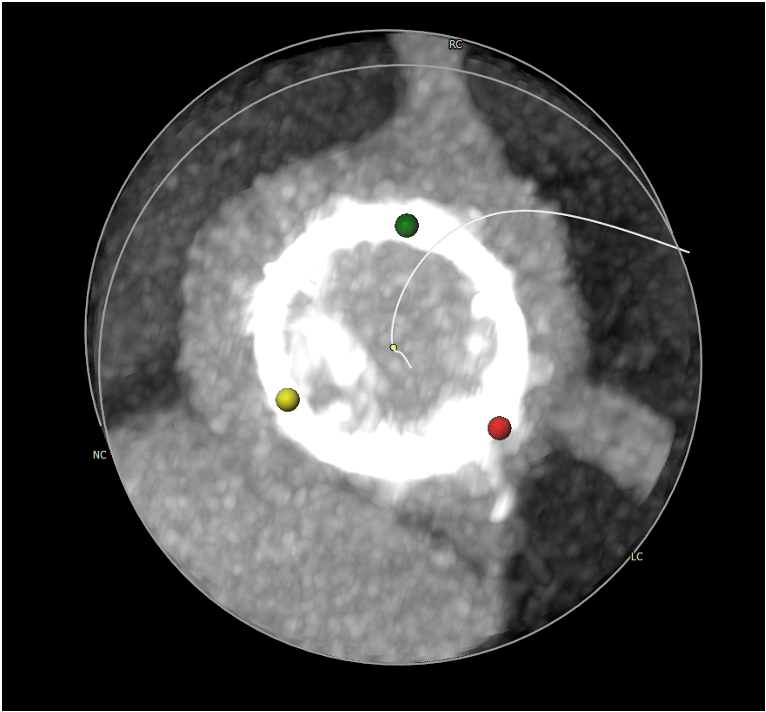
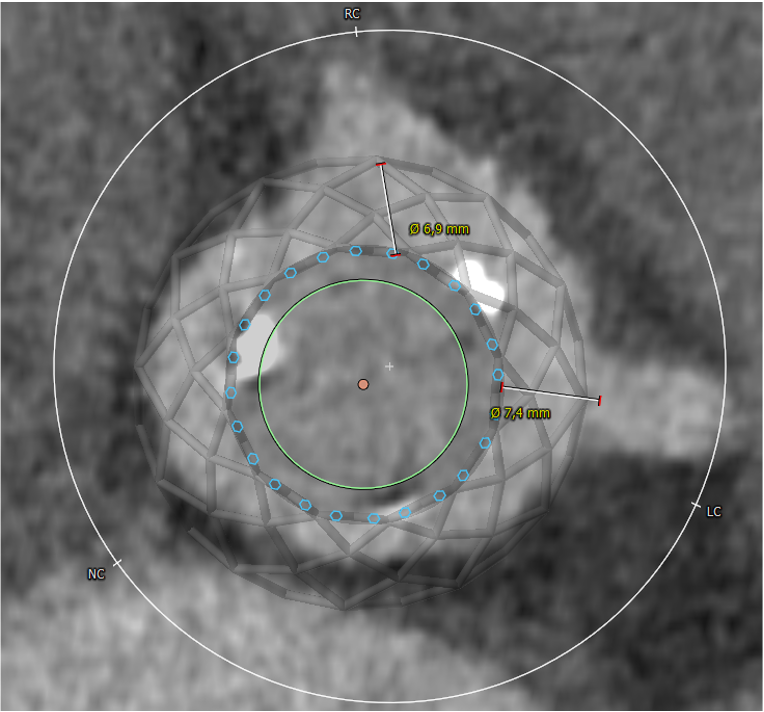
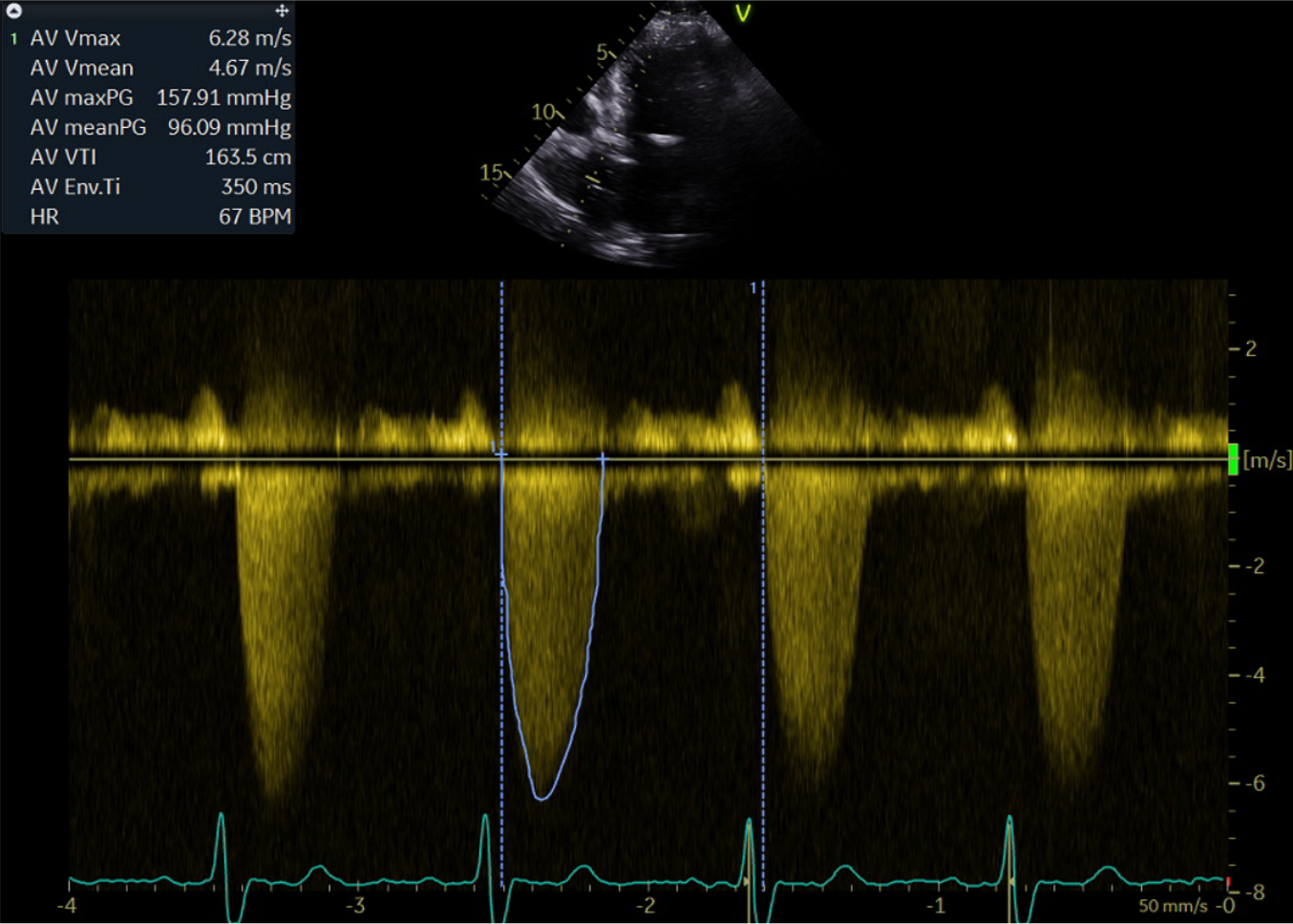
Transthoracic echocardiography showed a mean trans-prosthetic gradient of 86 mm Hg and pre-procedural cardiac computed tomography revealed heavily calcified bioprosthetic leaflets. VIV with a 23 mm Evolut�� R valve under local anesthesia was planned.
Relevant Catheterization Findings
After placement of a Sentinel device (Boston Scientific, MA, USA) for cerebral embolic protection, multiple catheters and guidewires were attempted, but all failed to cross the severely stenotic surgical bioprosthetic aortic valve. Given the uncrossable surgical aortic bioprosthesis, an antegrade approach to cross the aortic valve was considered – and this in local anesthesia.
 video 1.mp4
video 1.mp4
video 2.mp4
video 3.mp4
Interventional Management
Procedural Step
First, a transvenous transseptal puncture was performed under guidance of intracardiac echocardiography, which was introduced in the right atrium. Next, an 8.5 F Agilis�� NxT steerable introducer (Abbott Vascular, CA, USA) was introduced into the left atrium over a stiff guidewire which was placed in the left upper pulmonary vein. Through this steerable introducer, a 6 F pigtail catheter was placed into the left ventricle (LV). A standard exchange length (260 cm) J-tipped guidewire was then introduced into the pigtail catheter and was able to cross the surgical aortic bioprosthesis in an antegrade fashion. The guidewire was successfully snared in the descending aorta using an Amplatz Goose Neck�� snare and externalized from the 14 F arterial introducer sheath at the right femoral artery. An arterial-venous (A-V) loop was then formed and a 6 F pigtail catheter was introduced through this A-V loop from the arterial sheath and advanced through the surgical aortic bioprosthesis retrogradely into the LV. Both the guidewire and the antegrade pigtail catheter were subsequently removed together with the steerable introducer from the venous system. A standard TAVR procedure was then performed. After predilatation with an 18 mm True Dilatation balloon, the transcatheter heart valve was successfully implanted with no significant peri-device leak and an invasively measured gradient of 5 mmHg.
video 4.mp4
video 5.mp4
video 6.mp4
Case Summary
In conclusion, the antegrade-retrograde technique and A-V loop formation are widely applied techniques in the field of coronary chronic total occlusion and congenital heart procedures. This case illustrates that this technique can also be useful as a bailout solution in uncrossable aortic bioprosthesis during VIV-TAVR, especially when standard methods fail.
|
AP VALVES & SH 2021 Virtual Aug 05, 2021
|
|
| Thankfulness to you for sharing that very knowledge of yours with all of us! | |