
CASE20210512_001
Presenter
Rajaram Anantharaman
Authors
Rajaram Anantharaman1, Sandhya Sundararajan
Affiliation
Kauvery Hospital, India1
Structural Heart Disease - Congenital Heart Disease (ASD, PDA, VSD)
Hybrid Repair of A Complex Congenital Heart Disease Incomplete Shone Complex
Rajaram Anantharaman1, Sandhya Sundararajan
Kauvery Hospital, India1
Clinical Information
Patient initials or Identifier Number
AP
Relevant Clinical History and Physical Exam
28-year-old male with Incomplete Shone complex consisting of severe Juxtaductal coarctation of aorta and Supra mitral ring causing moderate to severe mitral stenosis. He also had additional mid muscular ventricular septal defects and patent ductus arteriosus with moderate pulmonary artery hypertension and atrial fibrillation.
Relevant Test Results Prior to Catheterization
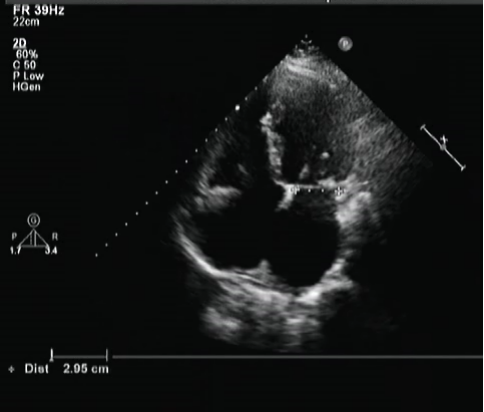
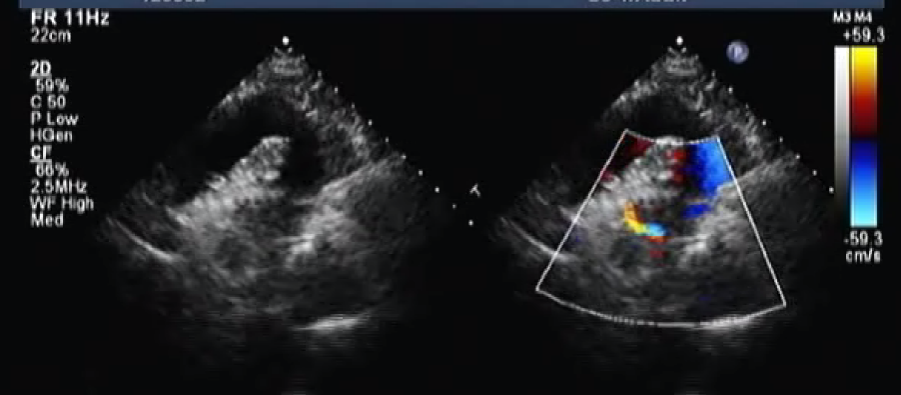
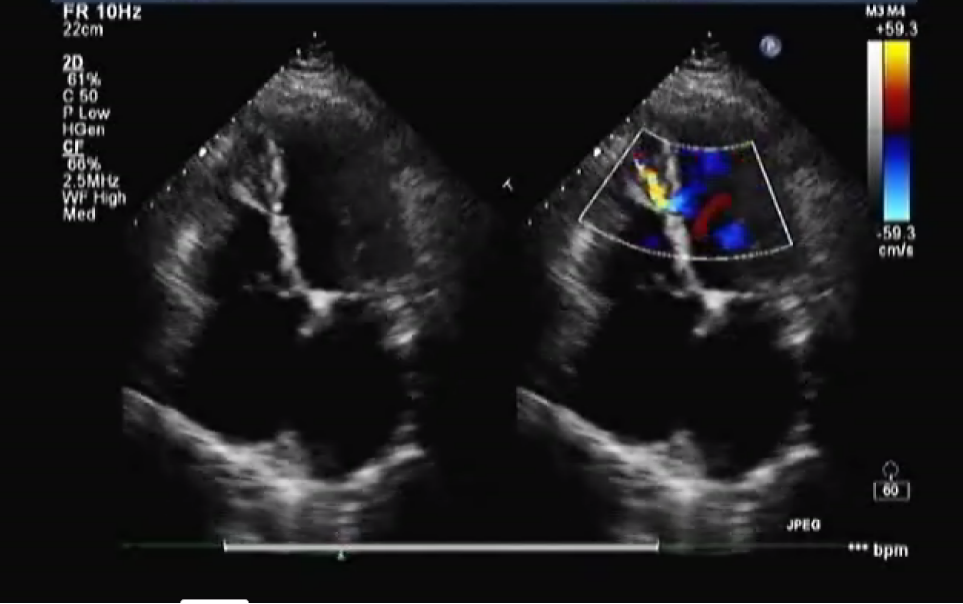
Pre-operative echo showed incomplete Shone complex consisting of supramitral ring & Aortic coarctation with muscular VSD & PDA
Relevant Catheterization Findings
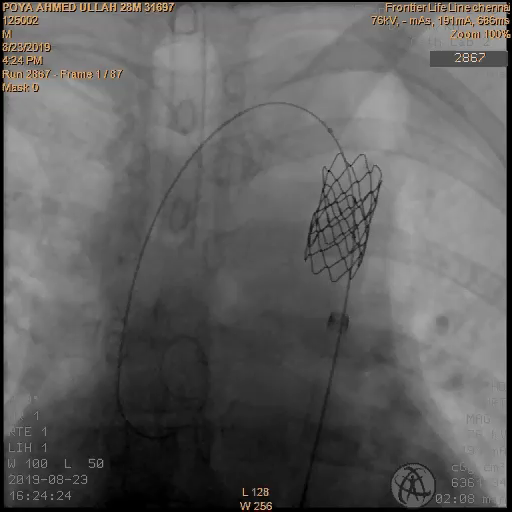
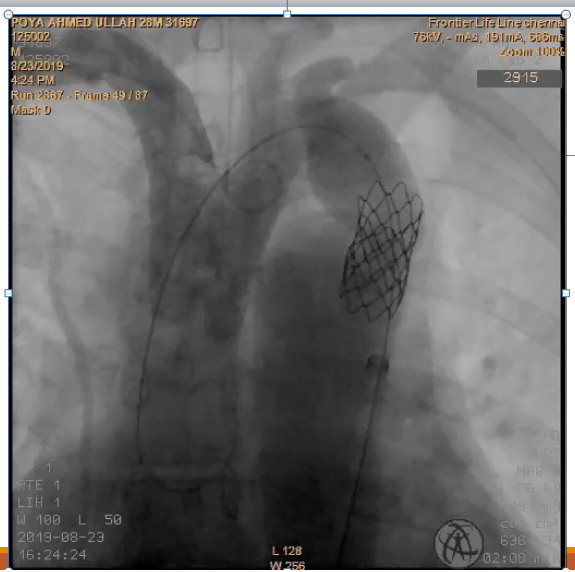
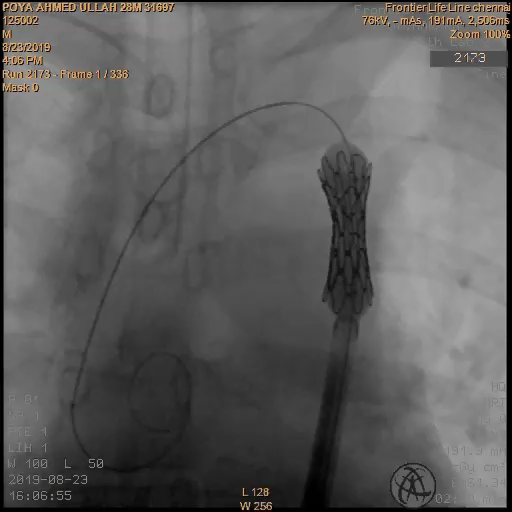
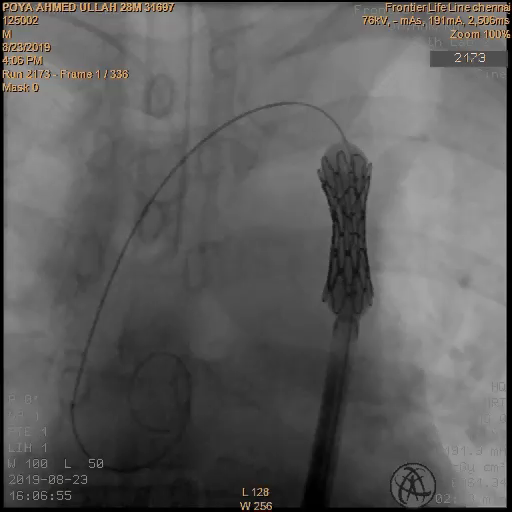
Procedure done: Hybrid stent placement for coarctation of aorta with 14 x 40 mm covered mounted CP stent followed by surgical resection of the supramitral ring, closure of VSD and left atrial appendage closure.

Interventional Management
Procedural Step
Through right femoral artery access, coarctation could not be crossed. Hence, using right brachial artery access, 5F pigtail catheter was placed in aortic arch & angiogram done showed Coarctation segment. Antegrade crossing of coarctation was done with 0.035�� Terumo wire and snared through femoral artery access. 5F MPA catheter was inserted and crossed the coarctation point.

Case Summary
We have performed a single stage hybrid repair of aortic coarctation stenting followed by surgical correction of mitral valve anomaly and ventricular septal defects. The simultaneous approach enabled us to undertake this complex surgical case with reduced peri operative risk. Hybrid procedures reduce duration and complexity of surgery, shortens the cardiopulmonary bypass time, avoids requirement for secondary surgery, reduces post-operative complications and hospitalization time. Hybrid repair can be considered as a successful and safe alternative for treating complex congenital heart disease.
|
AP VALVES & SH 2021 Virtual Aug 05, 2021
|
|
| Very good observation! It's very helpful for us. | |