
CASE20210512_002
Presenter
Rajaram Anantharaman
Authors
Rajaram Anantharaman1, Sandhya Sundararajan, RAGHAVAN SUBRAMIANIAN
Affiliation
Kauvery Hospital, India1
Valve - Others
Transcatheter Closure of a Large Post Bentall Ascending Aortic Psedoaneurysm
Rajaram Anantharaman1, Sandhya Sundararajan, RAGHAVAN SUBRAMIANIAN
Kauvery Hospital, India1
Clinical Information
Patient initials or Identifier Number
AB
Relevant Clinical History and Physical Exam
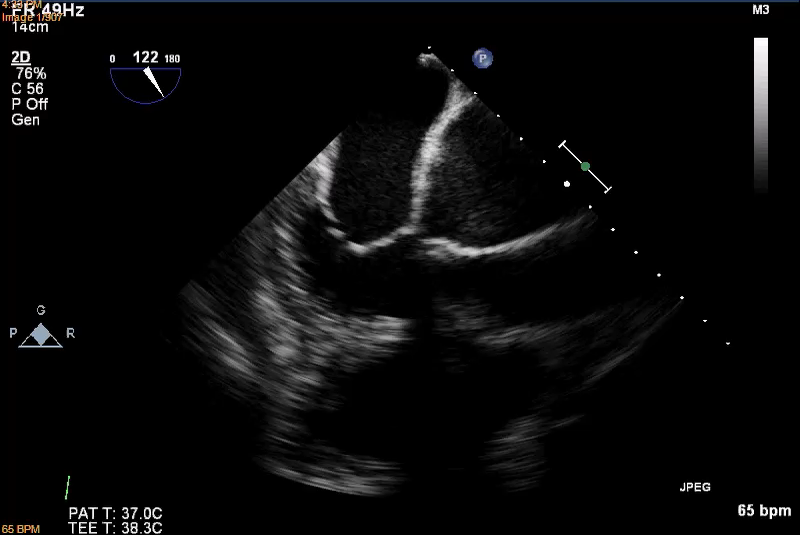
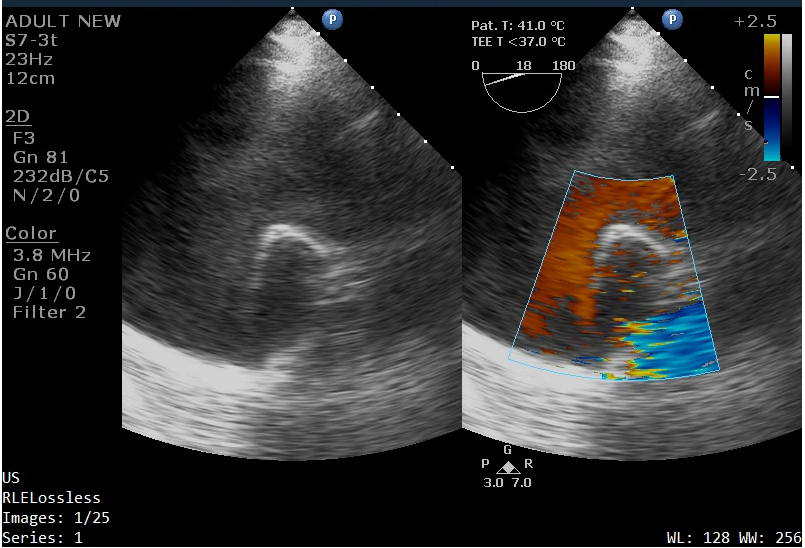
A 44 year old male was diagnosed with severe aortic regurgitation and ascending aorta aneurysm in July 2012. He underwent Bentall��s procedure with composite 23mm St. Jude Mechanical valve & 26mm collagen coated Dacron graft. He was asymptomatic for the past 7 years and had defaulted follow up. Echocardiogram revealed a normally functioning mechanical valve in the aortic position and a large pseudoaneurysm around the ascending aorta graft (Figures 1 & 2).
Relevant Test Results Prior to Catheterization
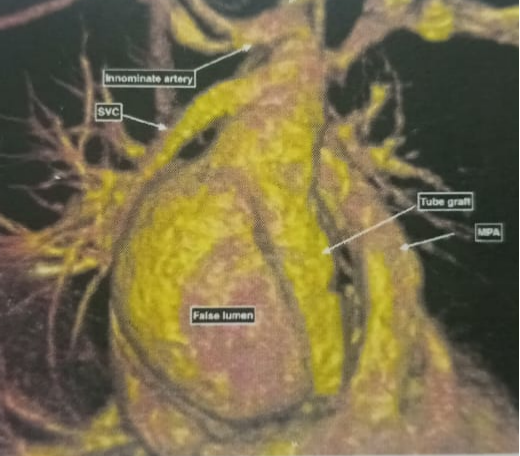
Cardiac MRI demonstrated a fistulous communication 1.5 x 1.8 cm between the true and false lumen at the posterior aspect of the distal anastomotic site leading to a large pseudoaneurysm of size 5.5cm around the ascending aorta graft (Figure 3).
Relevant Catheterization Findings
The diagnosis of ascending aorta pseudoaneurysm was confirmed by cardiac MRI. This case was discussed in a multidisciplinary meeting with our heart team. The MRI had demonstrated the distal anastomotic site leak into a large pseudoaneurysm through a fistulous tract which was amenable to device closure. Aortic re-operation is associated with high mortality and morbidity. Hence, decision was taken to proceed with percutaneous repair of the aortic pseudoaneurysm.
Interventional Management
Procedural Step
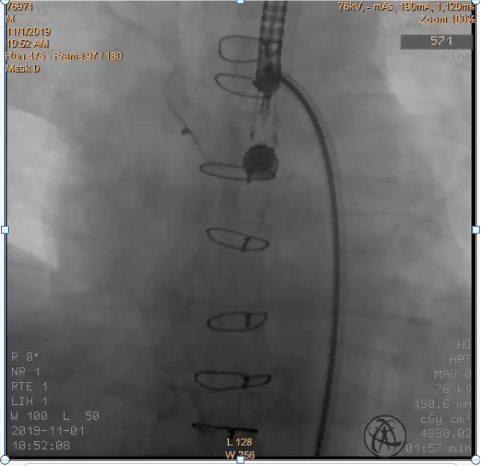
The procedure was done under general anaesthesia with transesophageal echocardiogram guidance. Right and left femoral arterial access was obtained using modified Seldinger technique. The right common femoral artery was pre-closed with a 6F Perclose ProGlide and upsized to a 10 F sheath. A 6 F sheath was placed in the left common femoral artery. A 5 F Pigtail catheter was advanced through the left common femoral artery and placed in the aortic root. Angiogram demonstrated the ascending aorta pseudoaneurysm (Figure 4). Transesophageal echo showed the pseudoaneurysm with a 16 -18 mm defect in the posterior aspect of the aortic wall.

Case Summary
This case demonstrates the successful percutaneous repair of a pseudoaneurysm of the ascending aorta post cardiac surgery using an ASD occluder device. We emphasize the importance of a multidisciplinary heart team approach to decide the best treatment plan for the patient. Redo surgery is associated with high morbidity and mortality. Endovascular stent grafting requires satisfactory landing zones for anchoring. Percutaneous options like placing a covered stent across the neck, device closure and coiling of the pseudoaneurysm sac should be considered. Percutaneous device closure is a low risk suitable alternative procedure in these patients.
|
AP VALVES & SH 2021 Virtual Aug 05, 2021
|
|
| Top-notch work! We��ve learned a lot from you! | |