
CASE20210512_003
Presenter
Tomonobu Yanase
Authors
Tomonobu Yanase1, Mizuki Miura1, Jiro Ando1, Haruo Yamauchi1, Issei Komuro1
Affiliation
The University of Tokyo Hospital, Japan1
Valve - Aortic Valve
Successful Transfemoral TAVR Using SAPIEN 3 for Bicuspid Aortic Valve Stenosis
Tomonobu Yanase1, Mizuki Miura1, Jiro Ando1, Haruo Yamauchi1, Issei Komuro1
The University of Tokyo Hospital, Japan1
Clinical Information
Patient initials or Identifier Number
K.N.
Relevant Clinical History and Physical Exam
A 68-year-old man with coronary artery disease and intestinal tumor presented with dyspnea (NYHA II) and he needed early surgery for intestinal tumor accompanied by bleeding. Transthoracic echocardiography (TTE) revealed severe aortic valve stenosis (AS). Computed tomography (CT) revealed the anatomy was feasible for transfemoral transcatheter aortic valve replacement (TAVR). We planned transfemoral TAVR to perform the surgery for the tumor immediately.
Relevant Test Results Prior to Catheterization
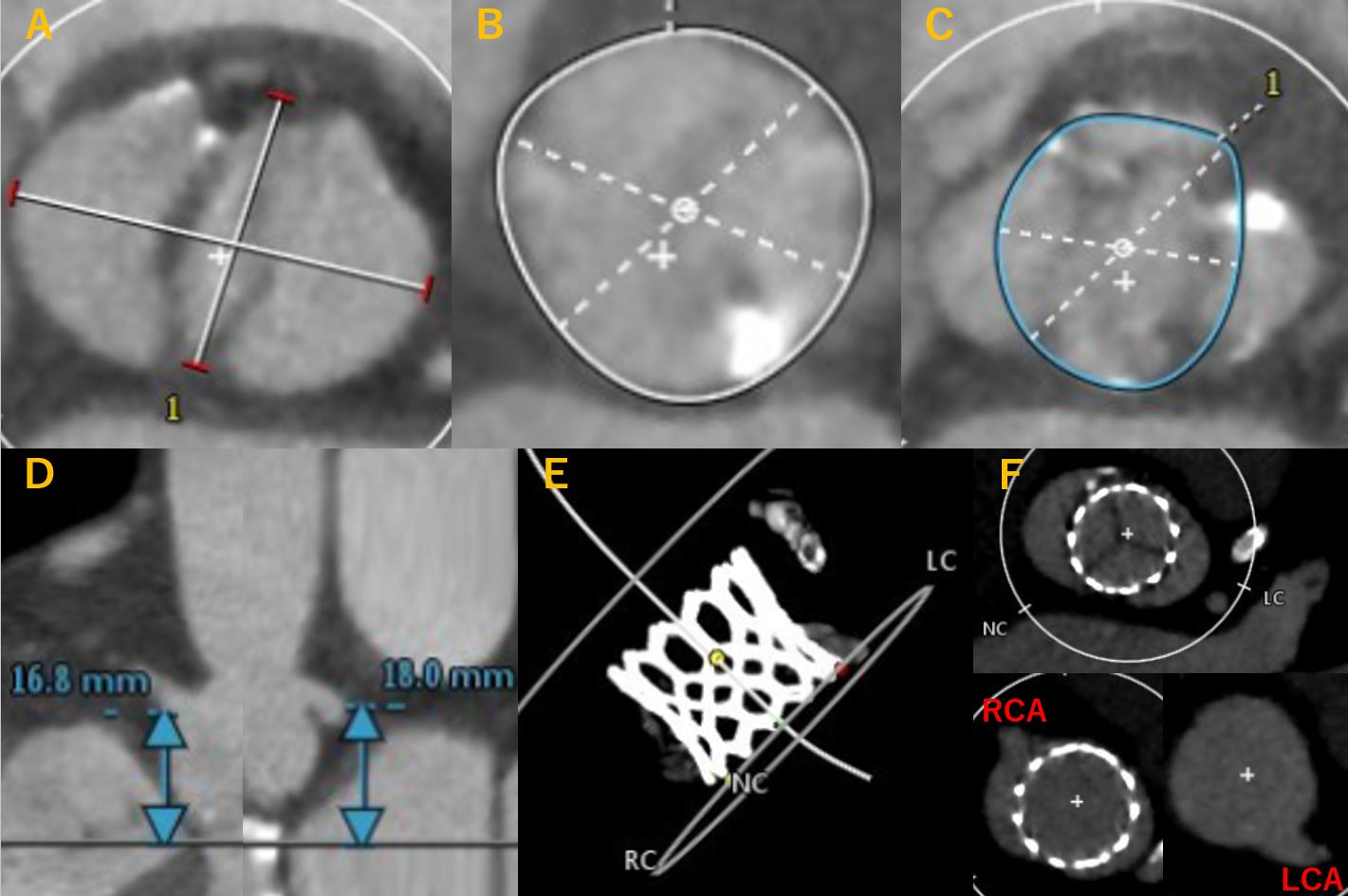
TTE revealed severe AS with a peak transaortic jet velocity of 4.2 m/s and mean transvalvular gradient of 43 mmHg. The Society of Thoracic Surgeons (STS) predicted risk of operative mortality (PROM) was 3.7%. Type 0 bicuspid AS was detected in CT (Figure 1A). CT angiogram images revealed an annulus area of 440.7 mm2 (Figure 1B). In the device landing zone, area of expected spread was 410.8 mm2, and minimum diameter of it was 21.7 mm (Figure 1C). Coronary height was normal (Figure 1D).
Relevant Catheterization Findings
Aortography showed a bicuspid AS. Coronary angiography showed no significant coronary stenosis including a previously implanted stent in the left anterior descending artery.
Interventional Management
Procedural Step
We selected balloon-expandable SAPIEN 3 (Edwards Lifesciences, Irvine, CA, USA) because of his age and the anatomy. SAPIEN 3 enables to access to coronary artery easily after TAVR, and it is better to access to the coronary artery after TAVR, and it is easy to consider future transcatheter aortic valve (TAV)-in-TAV for failed prosthesis if the first TAV is SAPIEN 3.
SAPIEN 3 was implanted in nominal volume transfemorally without pre-dilation. We tried to implant it as high as possible (Video 1). The tips were in the followings; 1) slow inflation, 2) implant in the perpendicular view of SAPIEN 3, 3) lucent line technique. Aortography showed the optimal position of SAPIEN 3, and intraoperative echocardiography showed trivial paravalvular leak and the improvement of mean transvalvular pressure gradient as 5 mmHg. Post-procedural CT showed the optimal expansion of SAPIEN 3 without contained annulus rupture (Figure 1E), and no overlap between the coronary ostium and the TAV commissure (Figure 1F).
Case Summary
Even in the current era of refined TAVR, TAVR for a bicuspid AS in low-risk patients is still controversial and challenging. Our case demonstrated the successful case of TAVR for Type 0 AS using the SAPIEN 3.
|
AP VALVES & SH 2021 Virtual Aug 05, 2021
|
|
| Very grateful for sharing your knowledge with us! | |