
CASE20210512_004
Presenter
Nishant Gangil
Authors
Nishant Gangil1, Luke Tapp1, Thirumaran Rajathurai1, Lauren Deegan1
Affiliation
University Hospital Coventry and Warwickshire NHS Trust, United Kingdom1
Valve - Aortic Valve
Transfemoral Transcatheter Aortic Valve Implantation in Rheumatic Aortic Stenosis with Pre-exisiting Mechanical Mitral Prosthesis
Nishant Gangil1, Luke Tapp1, Thirumaran Rajathurai1, Lauren Deegan1
University Hospital Coventry and Warwickshire NHS Trust, United Kingdom1
Clinical Information
Patient initials or Identifier Number
PC
Relevant Clinical History and Physical Exam
Clinical History:58 year old femalePrevious Mechanical Mitral Valve replacement 1992 with Bjork Shiley Prosthesis for Rheumatic Mitral stenosisRheumatic severe aortic stenosis and moderate aortic regurgitationNYHA III dyspnoeaType 2 DiabetesAtrial fibrillation
Physical Examination:Wt 57kg Normal BMIElevated JVP Bilateral pitting pedal edemaVariable S1 Mechanical Click audibleHarsh ejection systolic murmur in aortic area radiating to apex and carotidsBilateral basal lung crepts
Physical Examination:Wt 57kg Normal BMIElevated JVP Bilateral pitting pedal edemaVariable S1 Mechanical Click audibleHarsh ejection systolic murmur in aortic area radiating to apex and carotidsBilateral basal lung crepts
Relevant Test Results Prior to Catheterization
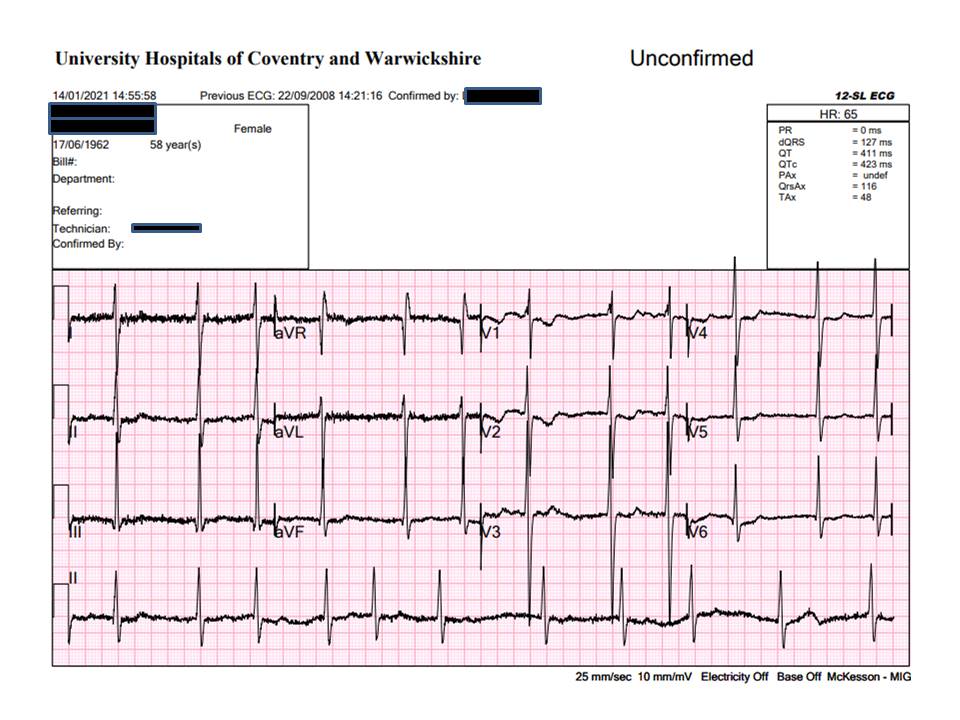
A. 12-lead Electrocardiogram: Atrial Fibrillation, ventricular rate of 66bpm, normal QRS duration with right axis deviation.
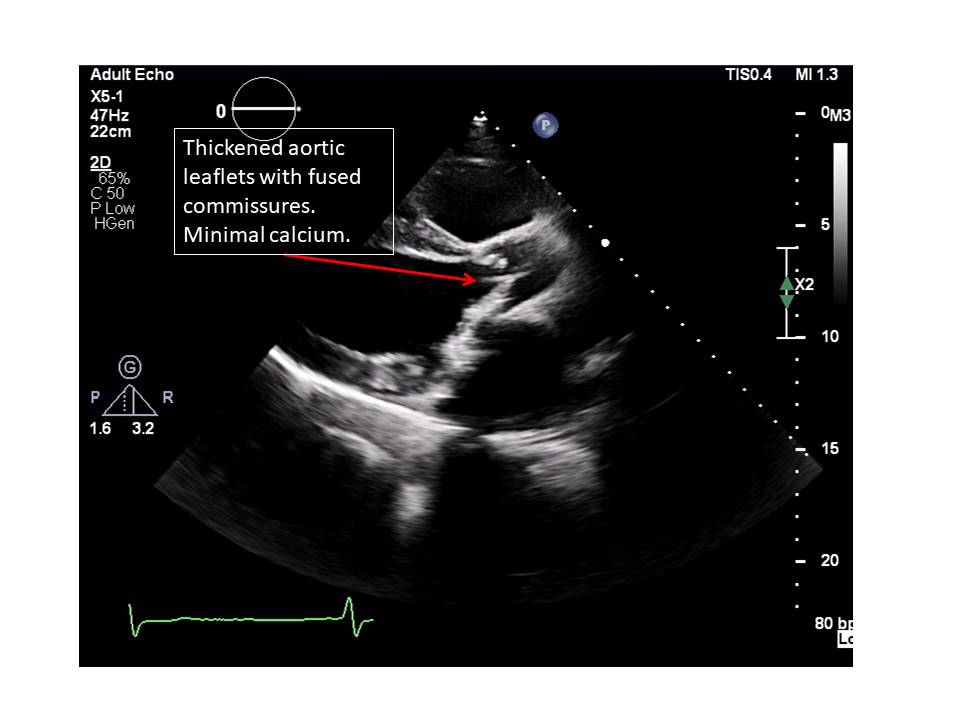
B. Transthoracic Echocardiogram: Rheumatic aortic valve with severe aortic stenosis and moderate regurgitation.Peak gradient 70mmHg Mean gradient 40mmHg. Aortic valve area 0.83cm2 . Normal mitral valve prosthesis.Severe global LV dysfunction. LVEF 30%
C. Chest X-Ray: Cardiomegaly with cephalisation of upper lobe pulmonary veins. Mechanical mitral prosthesis in-situ.
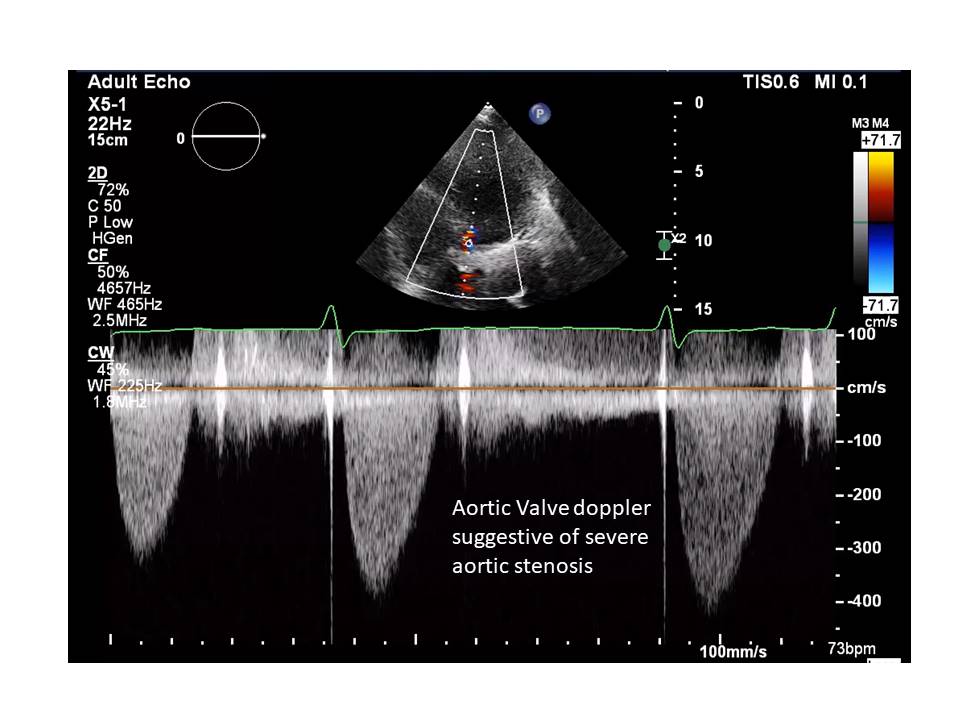
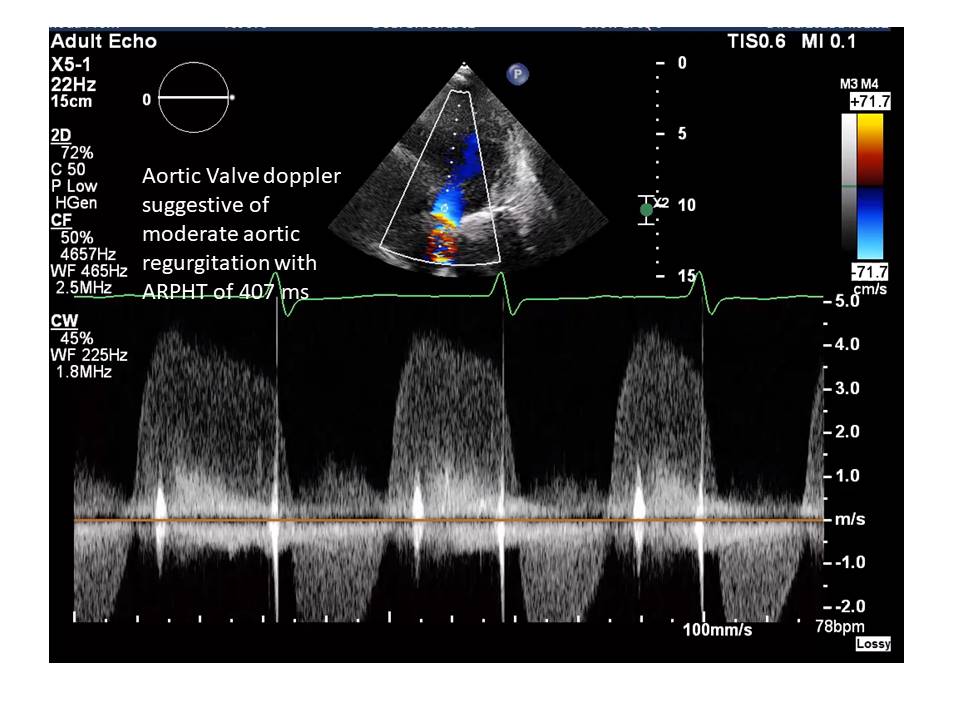

B. Transthoracic Echocardiogram: Rheumatic aortic valve with severe aortic stenosis and moderate regurgitation.Peak gradient 70mmHg Mean gradient 40mmHg. Aortic valve area 0.83cm2 . Normal mitral valve prosthesis.Severe global LV dysfunction. LVEF 30%
C. Chest X-Ray: Cardiomegaly with cephalisation of upper lobe pulmonary veins. Mechanical mitral prosthesis in-situ.
Relevant Catheterization Findings
A. Invasive Coronary Angiogram: Normal coronaries with no obstruction.
B. TAVI CT Scan: Agatson score of aortic valve: 30Rheumatic tricuspid aortic Valve with area of 505mm2 and perimeter of 84mm. Spacious sinus of valsalva 34x33x32 mm.LCA height 15mm RCA height of 21mm. No LVOT calcium. Good sized peripheral arteries with no significant luminal obstruction or calcium.Mitral prosthesis in situ (Bjork Shiley tilting disc valve).Aorto-mitral distance 8mm
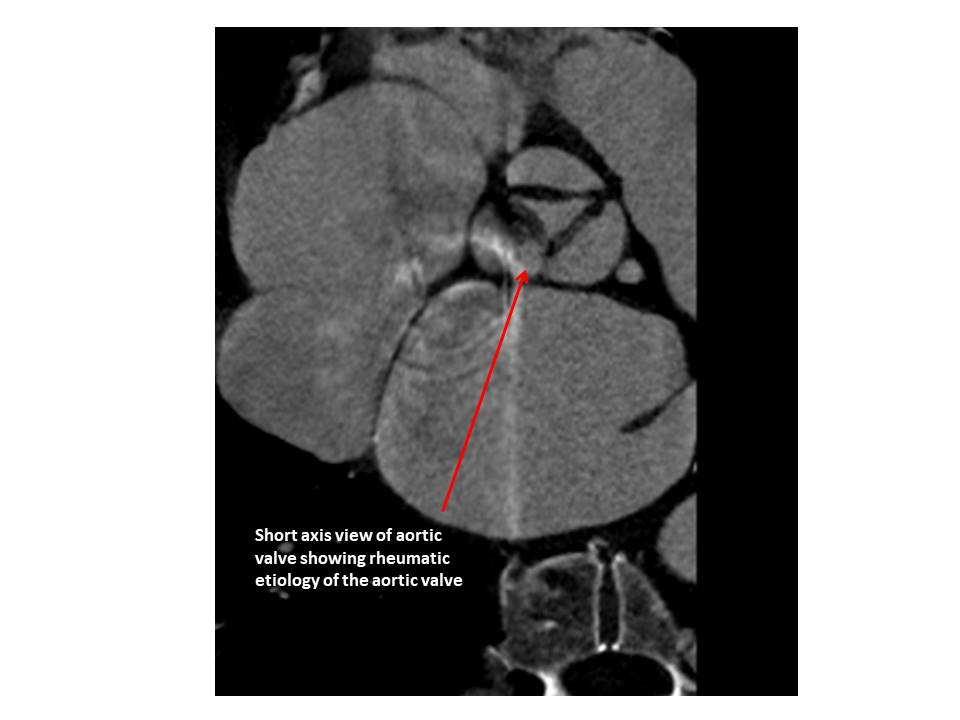

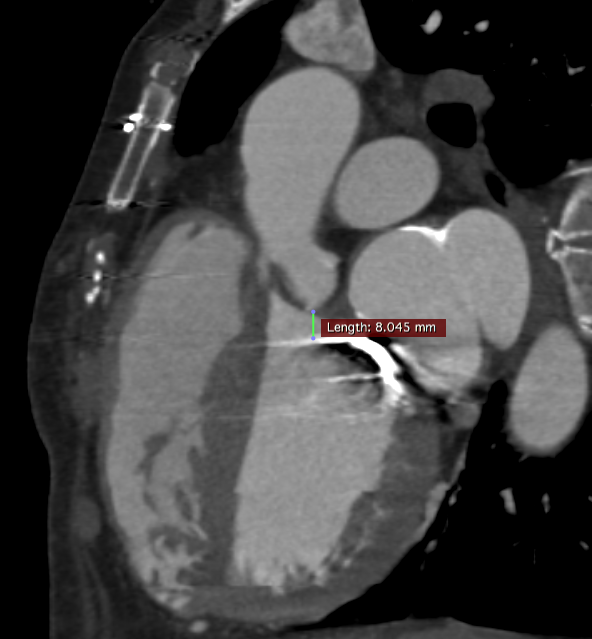
B. TAVI CT Scan: Agatson score of aortic valve: 30Rheumatic tricuspid aortic Valve with area of 505mm2 and perimeter of 84mm. Spacious sinus of valsalva 34x33x32 mm.LCA height 15mm RCA height of 21mm. No LVOT calcium. Good sized peripheral arteries with no significant luminal obstruction or calcium.Mitral prosthesis in situ (Bjork Shiley tilting disc valve).Aorto-mitral distance 8mm
Interventional Management
Procedural Step
There were three important technical decisions:A. Balloon expandable vs self expanding valve: Low calcium score of aortic valve would favour TAVI with balloon expanding valve (BEV) as it can be overinflated to get good anchorage around aortic annulus. Infact, there are number of case reports, where BEV has been used in isolated aortic regurgitation with non-calcific aortic valve. However, in this case it was important to have the advantage of recapturability as there was risk of interfering with mechanical mitral valve prosthesis. Therefore, decision was made to use Medtronic Evolut R Self expanding prosthesis for TAVI.
B. Sizing of TAVI prosthesis: Even though perimeter of 84mm comes in the range of 34mm Evolut R valve, considering that she was barely 5 feet tall, plan was to make decision between 29mm Evolut R Pro vs 34mm Evolut after aortogram and predilatation with 25mm Nucleus Balloon.
C. Aorto-mitral distance: In our experience, a minimum 5mm distance of aorto-mitral distance is required to safely implant a TAVI prosthesis in presence of mechanical mitral valve.
Procedural steps:Access was gained under ultrasound guidance. Balloon aortic valvuloplasty done with 25 mm Nucleus balloon. (Video 1)Both on aortogram and during valvuloplasty, it was felt that a 29mm Evolut R Pro valve would be more suitable. Also, the skirt of Pro valve would help in mitigating any paravalvular aortic regurgitation.Valve deployed successfully (Video 2)Excellent final result (Video 3)
 Predilatation with 25mm Nucleus balloon.mov
Predilatation with 25mm Nucleus balloon.mov
Valve opening under pacing.mov
Pre release Angiogram.mov
Very slow valve release.mov
Final Angiogram.mov
B. Sizing of TAVI prosthesis: Even though perimeter of 84mm comes in the range of 34mm Evolut R valve, considering that she was barely 5 feet tall, plan was to make decision between 29mm Evolut R Pro vs 34mm Evolut after aortogram and predilatation with 25mm Nucleus Balloon.
C. Aorto-mitral distance: In our experience, a minimum 5mm distance of aorto-mitral distance is required to safely implant a TAVI prosthesis in presence of mechanical mitral valve.
Procedural steps:Access was gained under ultrasound guidance. Balloon aortic valvuloplasty done with 25 mm Nucleus balloon. (Video 1)Both on aortogram and during valvuloplasty, it was felt that a 29mm Evolut R Pro valve would be more suitable. Also, the skirt of Pro valve would help in mitigating any paravalvular aortic regurgitation.Valve deployed successfully (Video 2)Excellent final result (Video 3)
Case Summary
t1. Rheumatic aortic stenosis can be successfully treated with trans-catheter aortic valve implantation after careful planning.
2. TAVI can be performed safely in the presence of mechanical mitral valve prosthesis.
3. In complex cases, choice of TAVI prosthesis should be based on CT findings, patient's clinical features, body habitus and behaviour of balloon during predilatation.
4. In our experience, rheumatic aortic stenosis behaves like bicuspid aortic valve during TAVI and therefore slightly undersized valve can considered. Valve is constrained at leaflet level rather than annular level.
5. Controlled pacing is extremely important while deploying the valve.
|
AP VALVES & SH 2021 Virtual Aug 05, 2021
|
|
| Thankfulness actually for your knowledge sharing! | |