
CASE20220611_001
Cryptogenic Stroke Presenting with Seizures in A 24 Year Old Filipino Female , A Case of Patent Foramen Ovale
By Cristina Sarmiento Tabucan
Presenter
Cristina Sarmiento Tabucan
Authors
Cristina Sarmiento Tabucan1
Affiliation
Philippine Heart Center, Philippines1
Structural Heart Disease - Patent Foramen Ovale (PFO) Closure
Cryptogenic Stroke Presenting with Seizures in A 24 Year Old Filipino Female , A Case of Patent Foramen Ovale
Cristina Sarmiento Tabucan1
Philippine Heart Center, Philippines1
Clinical Information
Patient initials or Identifier Number
V.Z.
Relevant Clinical History and Physical Exam
Patient is a known case of Pulmonary Stenosis who had balloon valvotomy 8 years prior to admission. Interim was advised for TEE however she was unable to tolerate the procedure due to intraprocedural seizures and has lost to follow-up. She had recurrent headache and left sided body weakness for a month with unremarkable CT scan. A 2D TTE done which showed a small Atrial Septal Defect. Interrogation using TEE was attempted but she had seizure recurrence intraprocedurally upon probe advancement.
Relevant Test Results Prior to Catheterization
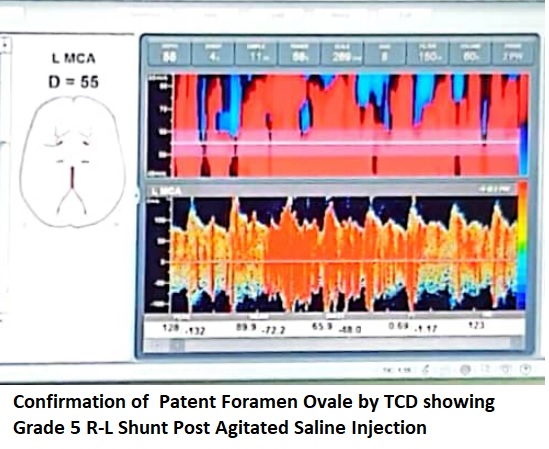
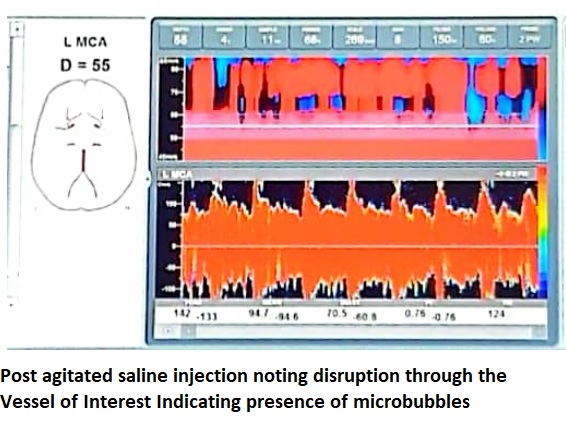
A small shunt in a young patient who had paradoxic stroke requires intervention. Our patient was unable to tolerate TEE under short acting sedation hence a Transcranial Dupplex Ultrasound was done to confirm the presence of a possible R-L shunt causing venous microemboli to cross the arterial system. Grade 5 right to left shunt and blips were detected upon injection of agitated saline during valsalva confirming presence of a Patent Foramen Ovale instead of the previously considered ASD.
Relevant Catheterization Findings
Interventional Management
Procedural Step
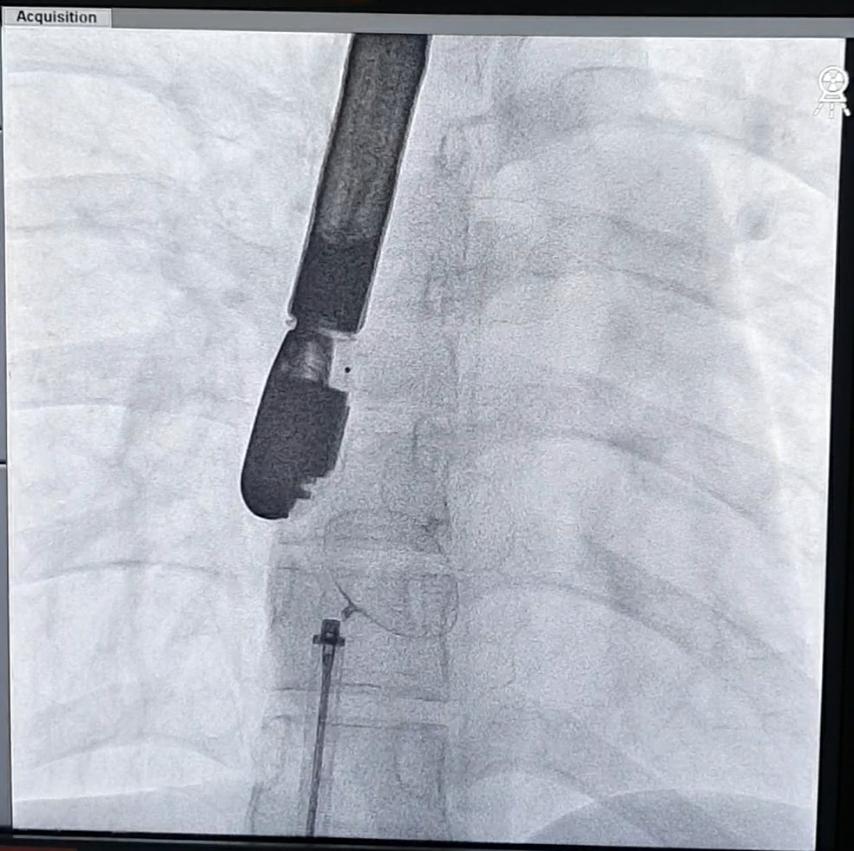
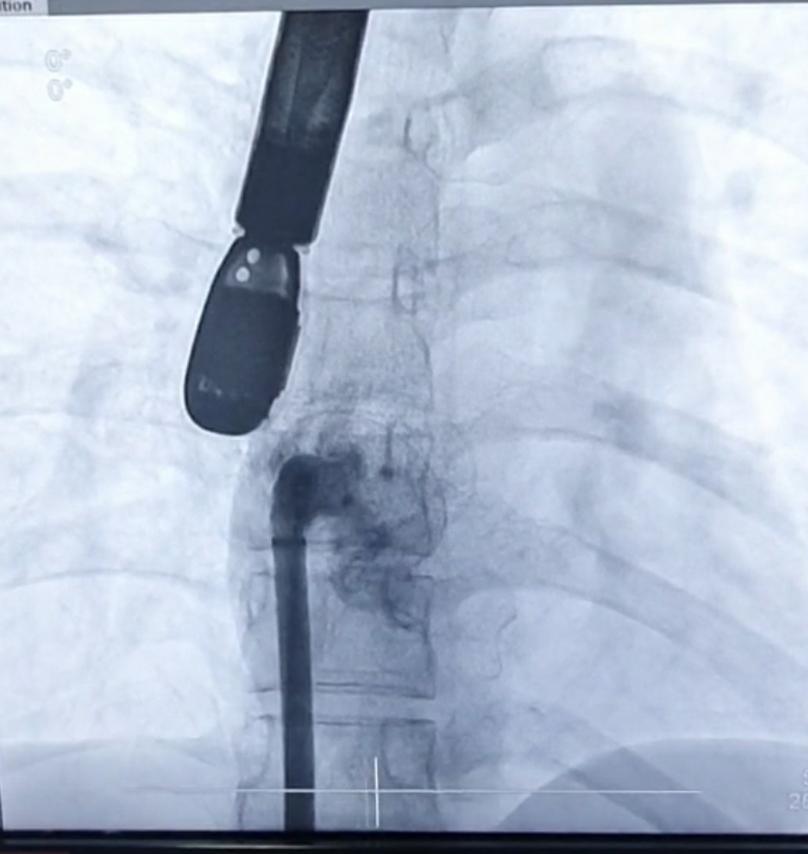
The team decided to do a transcatheter device closure approach for this patient. She was placed on IV and gas sedation to prevent recurrence of intraprocedural seizures during the placement of TEE probe. Femoral venous sheath was placed for access while a multipurpose wire was inserted to outline the left atrium. Using a 6-F catheter, a guidewire was advanced to the PFO. A PFO occluder device size 30mm was successfully deployed. After device release, an angiogram was done confirming correct placement of the device implanted. A post-procedural transesophageal echocardiogram was then facilitated showing no residual shunts post deployment of the device.
Case Summary
Patent foramen ovale remains the most common cause of cryptogenic stroke in the young and may also cause recurrent migraine headache especially in a otherwise healthy individual. Paradoxic emboli results from a right to left shunting due to the patent conduit allowing microemboli passage from venous to the arterial system. The risk for recurrent stroke occurs in 6-8% of an unrepaired PFO and therefore warrants closure. TEE remains the gold standard to its diagnosis however in a patient where TEE cannot be done such as in our patient who experiences recurrent seizures intraprocedurally, transcranial doppler ultrasound provides an alternative for its confirmation and diagnosis.