
CASE20220612_001
Salvaging hopeless patient with AS, chronic refractory heart failure, liver and kidney failure, and prolonged resuscitation during TAVI
By Teguh Santoso, Linda Lison
Presenter
Teguh Santoso
Authors
Teguh Santoso1, Linda Lison1
Affiliation
Medistra Hospital, Indonesia1
Valve - Aortic Valve
Salvaging hopeless patient with AS, chronic refractory heart failure, liver and kidney failure, and prolonged resuscitation during TAVI
Teguh Santoso1, Linda Lison1
Medistra Hospital, Indonesia1
Clinical Information
Patient initials or Identifier Number
MN
Relevant Clinical History and Physical Exam
Male, 72 year old.
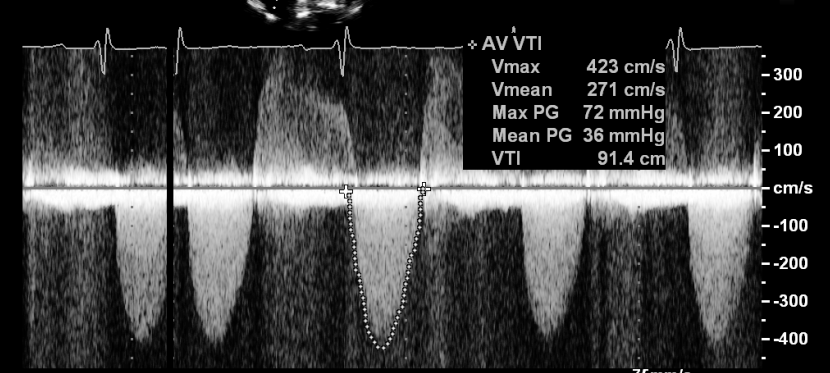
Relevant Test Results Prior to Catheterization
Severe, calcified AS, AVA 0.7 mm2, Max PG 72 mmHg, Mean PG 36 mmHg, VTI 91.4 cm/s, moderate AR, LV dilatation, EF 36%, moderate MR, MAC. EuroScore II 43.93%, STS risk for mortality 9.3%, risk of morbidity or mortality 41.6 %
 MN2.wmv
MN2.wmv
MN3.wmv
Relevant Catheterization Findings
Normal coronaries.
Interventional Management
Procedural Step
During deployment VF ensued, CPR was performed. Device redeployed but appeared constrained with a narrow transverse diameter and string sign indicating infolding of struts. Rigorous CPR performed. Finally after more than 62 minutes, heart responded to pacing. Hemodynamics became acceptable, pressure gradient 8 mmHg. No pulmonary edema. AR index 21. After TAVI patient had prolonged acute confusional state (for around 3 weeks) without other neurological sequels. Brain CT showed only age-related atrophy. However, 2.5 months later he began to show signs and symptoms of heart failure again. Echocardiogram showed max PG 35 mmHg, mean PG 20 mmHg. TEE demonstrated infolded valve, systolic flow convergence and AR. Decided to treat it. Rotational fluoroscopy showing the maldeployed valve. PPG across AoV 14 mmHg. Moderate AR. AR index 21. To avoid crossing the struts, the valve was crossed using a pigtail catheter & a 0.35” J-tip Terumo wire by prolapsing the wire across the valve. Balloon aortic valvuloplasty was done; resulting in mild AR, but with “normal” AR index (33). PPG 8 mmHg. TTE showed better expanded THV almost without infolding and no hemodynamic gradient across the valve. There was no annular hematoma or pericardial effusion post-procedure on echo. Liver and kidney function returned to normal as the derangement was “functional”. Patient was subsequently well, no symptom, could resume normal daily activities, NYHA 1, practically without neurological sequels.
MN4.wmv
MN5.wmv
MN6.wmv
Case Summary
A HOPE-less patient with AS, chronic refractory heart failure, liver and kidney failure, and prolonged resuscitation during TAVI is presented. After TAVI all the above medical problems gradually weaned off. He also had infolded valve which was treated with BAV with acceptable result. Never lose HOPE, because HOPE sees the invisible, feels the intangible, and achieves the impossible (Hellen Keller).