
CASE20220602_001
Heart-Hand Syndrome in a Young Adult Filipino
By Leica Mariz Balanon Royeca
Presenter
Leica Mariz Balanon Royeca
Authors
Leica Mariz Balanon Royeca1
Affiliation
Philippine Heart Center, Philippines1
Structural Heart Disease - Congenital Heart Disease (ASD, PDA, VSD)
Heart-Hand Syndrome in a Young Adult Filipino
Leica Mariz Balanon Royeca1
Philippine Heart Center, Philippines1
Clinical Information
Relevant Clinical History and Physical Exam
N.A. is a 25 years old male, Filipino who was acyanotic at birth. At 1 year old, he had pneumonia and a murmur was noted. 2ded showed PDA and bicuspid aortic valve. Surgical correction was advised but lost to follow-up.



Relevant Test Results Prior to Catheterization
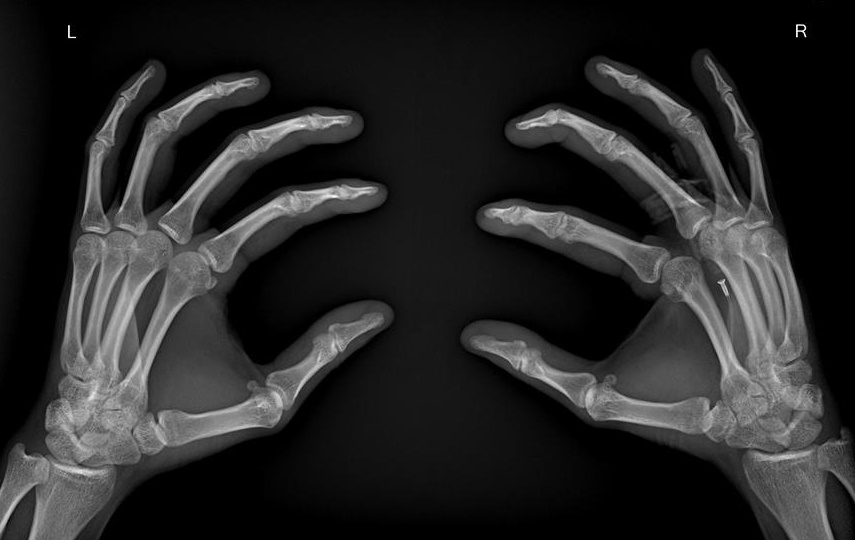
Hand xray: brachymetacarpia of the 2nd, 4th and 5th digits left
Pre op 2decho:
 BAV.mov
BAV.mov
PDA.mov
Pre op 2decho:
Relevant Catheterization Findings
Hemodynamic Studies and Coronary angiogram:
Interventional Management
Procedural Step
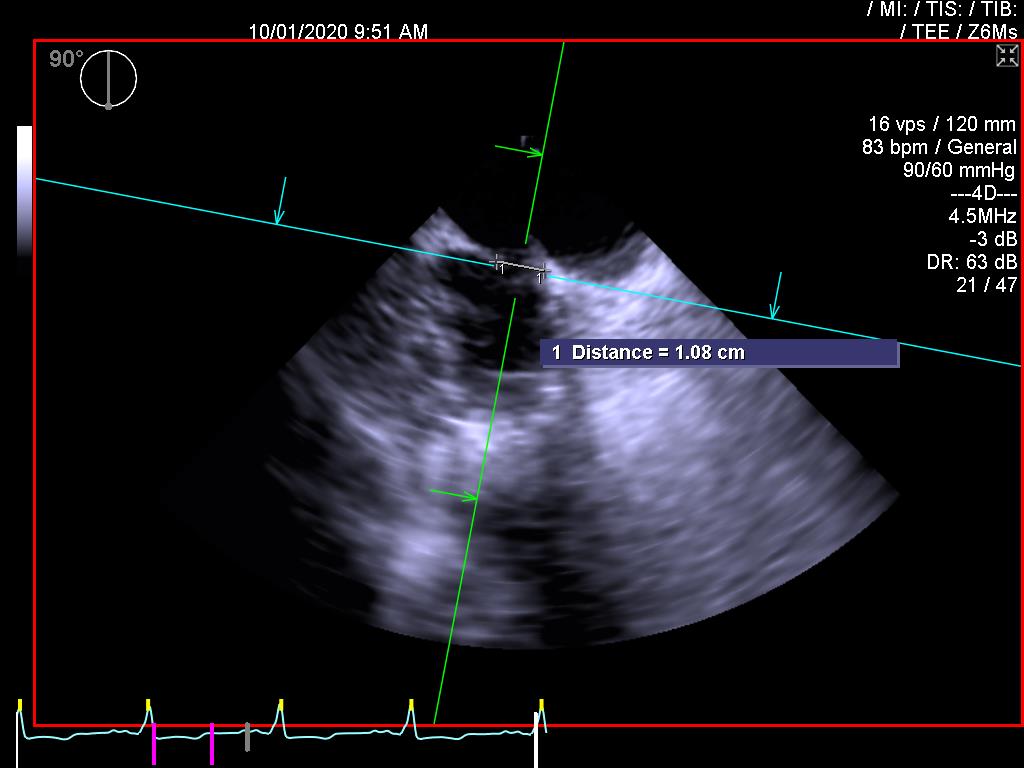
Patient was placed on supine position under GETA. Pre-operative transesophageal echocardiogram revealed a bicuspid aortic valve with fused noncoronary and right coronary cups. Mitral valve annulus was dilated at 5.3cm. Mid-line sternotomy done. Pericardium was opened and deflected. Aortic and bi-caval cannulation done. Left ventricular vent and antegrade plegia-line were placed. Cardiopulmonary bypass was initiated. Cross clamp applied and cardioplegia delivered. PDA dissected and isolated, then ligated proximally and distally. Posterior left atrial wall was opened. Mitral valve was inspected, annular sutures were placed, and annuloplasty ring was implanted. Left atrium was closed, aortotomy was done. Aortic valve was examined and resected, annular sutures were placed mechanical aortic valve was implanted. Aortotomy was closed. patient was rewarmed and weaned of bypass. Decannulation was done. JP drains placed in right pleura, left an right mediastinum. CTT was placed at anterior mediastinum. Anterior chest was closed in layers. Post-operative TEE showed a normally functioning mechanical aortic valve with no paravalvular leak. Residual shunt across the PDA was noted.
Pre-op TEE AoV.mov
IOTEE PDA.mov
Case Summary
Post-operative recovery was tolerated and uneventful. Patient was discharged with the following medications: Warfaring 5mg 1/2 tablet once daily, Sildenafil 25mg 1 tablet twice daily, Furosemide 40mg 1/2 tablet once daily and Spironolactone 50mg 1 tablet once daily. Upon follow-up at the outpatient department, patient reported improvement in functional capacity.